
Abstract
Given the global burden of psychotic disorders, the identification of patients with early-onset psychosis (EOP; that is, onset before the age of 18) at higher risk of adverse outcome should be a priority. A systematic search of Pubmed, Embase, and PsycInfo (1980 through August 2014) was performed to identify longitudinal observational studies assessing correlates and/or predictors of clinical, functional, cognitive, and biological outcomes in EOP. Seventy-five studies were included in the review. Using multivariate models, the most replicated predictors of worse clinical, functional, cognitive, and biological outcomes in EOP were premorbid difficulties and symptom severity (especially of negative symptoms) at baseline. Longer duration of untreated psychosis (DUP) predicted worse clinical, functional, and cognitive outcomes. Higher risk of attempting suicide was predicted by greater severity of psychotic illness and of depressive symptoms at the first episode of psychosis. Age at onset and sex were not found to be relevant predictors of outcome in most multivariate models, whereas studies using bivariate analyses yielded inconsistent results. Lower intelligence quotient at baseline predicted lower insight at follow-up, worse functional outcomes, and a diagnostic outcome of schizophrenia. Biological predictors of outcome in EOP have been little studied and have not been replicated. Lower levels of antioxidants at baseline predicted greater brain volume changes and worse cognitive functioning at follow-up, whereas neuroimaging markers such as regional cortical thickness and gray matter volume at baseline predicted remission and better insight at follow-up, respectively. EOP patients with poorer premorbid adjustment and prominent negative symptoms at initial presentation are at risk of poor outcome. They should therefore be the target of careful monitoring and more intensive interventions to address whether the disease course can be modified in this especially severely affected group. Early intervention strategies to reduce DUP may also improve outcome in EOP.
Similar content being viewed by others
Introduction
Neuropsychiatric disorders are the greatest contributor to global burden of disease in adolescents and young adults worldwide.1 There has been growing interest in prevention and early intervention in psychiatry in recent years,2,3 as it has become increasingly evident that effective management of child and adolescent psychiatric disorders can help prevent the development of persistent mental health concerns in adulthood4,5 and that early intervention strategies can positively impact long-term outcome of severe mental disorders, especially in young people.6–9
As neurodevelopmental disorders, schizophrenia and other psychoses usually show their first manifestations during childhood and adolescence, and 11–18% of patients present with their first episode of psychosis before age 18 (early-onset psychosis; EOP).10,11 Outcome in EOP is negatively affected by the impact of illness onset on individuals whose neurobiological and psychosocial development is not yet complete,12 leading to 50–60% of EOP patients with poor outcome.13 Although almost 40% of patients with schizophrenia will achieve social or functional recovery,14 and some will have a positive outcome even if medication is discontinued,15 there is still a large group of patients at risk of poor outcome. This group may constitute an even larger proportion in the population with an early-onset form of the illness, which makes identification of the risk factors associated with a poor outcome in this population especially valuable. This would facilitate more intensive and tailored interventions in those patients deemed to be at higher risk of having poor outcome, facilitating a rationalization of resources’ use and expectations.
Despite the interest of identifying predictors of outcome in this population, studies are still scarce and have shown contradictory results. One previous systematic review of predictors of outcome in adolescent first episode psychosis in papers published in 1989–1999 did not find any variable significantly predictive of diagnostic or overall outcome, except for (i) presence of abnormal premorbid personality traits, which was suggestive of a diagnostic outcome of schizophrenia, and (ii) lower functioning before and after the first episode of psychosis, which was associated both with a diagnostic outcome of schizophrenia and poorer overall outcome.16 Similarly, a more recent non-systematic review reported the following predictors of chronic long-term course in early-onset schizophrenia: younger age at illness onset, insidious onset, positive family history of non-affective psychosis, developmental delays, poor premorbid adjustment, longer duration of the first episode of psychosis, greater symptom severity and poorer psychosocial functioning at discharge, and higher number of relapses through follow-up.17
Given the potential clinical relevance of identifying predictors of outcome in children and adolescents with psychosis, we aimed to perform a comprehensive systematic review of the literature to date on predictors and correlates of clinical, functional, cognitive, and biological outcomes in EOP. We hypothesized that there would be a set of main predictors that overlap with those reported for adult-onset psychoses, and that those related to premorbid difficulties and developmental delays would play an especially important role in this population.
Materials and methods
Search strategy
A systematic two-step literature search was performed following the guidelines of the PRISMA statement.18 A Pubmed, Embase, and PsycInfo search (1980 through August 2014) was performed using the following search terms: (early-onset, childhood-onset, adolescent-onset, child*, adolescent*) combined with (psychosis, psychotic, schizophrenia, first-episode psychosis, first-episode psychotic, bipolar psychotic). In a second step, we manually reviewed the reference lists of the selected studies and previous reviews to identify any potentially relevant studies not identified by the computerized search.
The initial literature search yielded 3,750 studies and the manual search identified 47 additional studies. After removing duplicates, 2,293 potential studies were identified.
Selection criteria
The abstracts of the 2,293 resulting studies were assessed for eligibility using the following hierarchical criteria:
-
1
Studies were peer-reviewed original articles published in English.
-
2
Studies had a longitudinal and observational design. As the main objective of this review was to assess predictors and correlates of the course of EOP and not specific therapeutic interventions, studies assessing predictive and outcome variables in the context of a clinical trial were not included.
-
3
Participants had a diagnosis of schizophrenia or other psychotic disorders according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria - DSM-III, DSM-III-R, DSM-IV, DSM-IV-TR, or to the International Classification of Diseases (ICD) criteria - ICD-9 or ICD-10. This limitation was applied since, before the DSM-III, the definition of categories such as childhood-onset schizophrenia included clinical pictures that would currently be classified under the diagnostic category of autism spectrum disorders.19
-
4
Onset of psychotic illness in childhood or adolescence (that is, either the upper limit of the range of age at onset was <18 years or the onset was defined by the authors as a ‘childhood onset’, ‘adolescence onset’, and/or ‘early-onset’). In four studies, the upper limit of the range of the age at onset was >18, but mean age at onset or at baseline was <18 and the authors referred to these as participants with EOP.20–23 In two studies, the range of the age at onset or at baseline was not provided, but mean age at baseline was <18 and the authors referred to the sample as adolescent onset.24,25
-
5
Studies assessed clinical, functional, cognitive, and/or biological (that is, neuroimaging, biochemical) outcome measures or suicide risk. This broad definition of outcome was used to provide a more comprehensive perspective on the issue and to increase the clinical applicability of the results.
-
6
Studies assessed the association between demographic, clinical, functional, cognitive, and/or biological baseline variables and follow-up outcome measures using bivariate (for example, Student’s t-tests, analysis of variance, χ2-tests, correlations) or multivariate (for example, linear/logistic regression models or novel multivariate machine-learning methods) techniques.
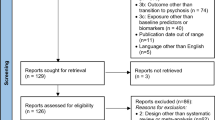
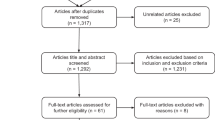
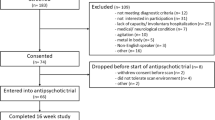
When the Abstract did not provide sufficient information to assess study eligibility, the full text was consulted. In instances where the full text was not available, the authors were contacted by e-mail. Of the 2,293 assessed studies, 214 full-text articles were selected and further assessed for eligibility. Of those, 75 studies fulfilled all the inclusion criteria and were ultimately included in the review. Figure 1 shows the flowchart of the literature review process.

Flowchart of study selection.
Data extraction
Data were extracted by two reviewers (CMD-C, AR-Q) and supervised by an external reviewer (LP-C). For each study, the following data were retrieved: author names, year of publication, name or acronym of the cohort, design (retrospective, prospective, or mixed), number of subjects, demographic variables (age at baseline, proportion of male subjects), clinical variables (age at onset, diagnosis distribution), length of follow-up, outcome measures, and predictors/correlates of outcome. Papers reporting on the same cohort were included as long as they provided additional information on any of the relevant outcome measures. Discrepancies were resolved by discussion.
Data synthesis and analysis
Studies were classified according to the type of outcome measures assessed (clinical, functional, cognitive, biological, or suicide risk), length of follow-up, and study cohort. For reporting purposes, findings are displayed (i) separately for studies using multivariate/regression models and those using bivariate analyses and (ii) only if associations/predictions reach a significance threshold of P<0.05.
Results
Table 1 provides a summary of the reported significant predictors (in studies using multivariate/regression models) or correlates (in studies using bivariate approaches) for each outcome category. For further description of the characteristics and main findings of the reviewed articles (for example, sample size, design, statistical methods, outcomes assessed), see Supplementary Table 1.
Using multivariate models, premorbid difficulties (that is, poorer premorbid adjustment, history of developmental disorder) and greater symptom severity (especially negative symptoms) at baseline were consistently found to be significant predictors of worse outcome across all areas (clinical, functional, cognitive, and neuroimaging). This is also true for studies using bivariate analyses (Table 1). A diagnosis of schizophrenia was a significant predictor of greater disability, lower global functioning, and poorer quality of life at follow-up. Longer duration of untreated psychosis (DUP) was a significant predictor of worse clinical, functional, and cognitive outcomes in multivariate models (Table 1). However, the association between DUP and clinical or functional outcomes was not replicated in an EOP sample with longer DUP using a bivariate approach.26
Although sex has not been found to be a relevant predictor in most studies using regression models,27–30 being female has been found to predict better insight and higher number of readmissions (see Table 1). In studies using bivariate approaches, being female has also been found to be associated with better global functioning, less likelihood of a chronic course and receiving clozapine, more likelihood of being in remission at follow-up, and less regional gray matter (GM) loss through follow-up (see Table 1). However, other studies have not found significant associations between sex and outcome.31,32
Lower age at onset has been found to predict worse quality of psychiatric care and poorer social, educational, and occupational functioning in multivariate models, but is not a consistently reported predictor of these and other outcomes in studies using regression models27,28,33 (Table 1). In bivariate studies, lower age at onset has been found to be associated with less likelihood of remission, worse global functioning, and greater disability, although there are also studies that do not find this association.31,34
Cognitive variables such as lower intelligence quotient (IQ) at baseline have been found to predict worse functional outcome, a diagnostic outcome of schizophrenia, or poorer insight at follow-up in multivariate models (Table 1).
Using multivariate models, biological predictors such as lower antioxidant levels at baseline have been found to predict greater brain volume changes and worse cognitive functioning at follow-up. Among neuroimaging markers, cortical thickness and GM volume at baseline in different brain regions have been found to predict remission and insight at follow-up, respectively (Table 1). However, other studies using multivariate techniques have not found significant associations/predictions between biological variables and outcomes such as diagnosis at follow-up in first-episode patients.35
Discussion
In this systematic review, we found that the most replicated predictors of worse clinical, functional, cognitive, and/or biological outcomes in EOP are a positive history of premorbid difficulties (developmental delays and poor premorbid adjustment), greater symptom severity (especially of negative symptoms) at baseline and longer DUP. Greater initial symptom severity is also a good predictor of attempting suicide during follow-up, together with greater severity of depressive symptoms at baseline or at discharge after the first episode. Cognitive variables such as lower IQ at baseline predict poorer insight at follow-up, worse functional outcomes, and a diagnostic outcome of schizophrenia. Biochemical variables such as lower blood antioxidant levels at baseline predict greater brain volume changes and worse cognitive functioning at follow-up, whereas regional brain thickness and volume measures of different brain regions at baseline predict remission status and insight at follow-up, respectively. Age at psychosis onset and sex do not seem to be consistent predictors of any outcome in EOP samples.
It has been proposed that developmental continuity may exist from premorbid difficulties to primary negative symptoms in EOP.36 The coexistence of severe premorbid impairments and negative symptoms delineate a large subgroup of EOP individuals with higher neurodevelopmental load who are eventually at risk of a deleterious course.37 This would be consistent with our finding that poorer premorbid adjustment and more prominent negative symptoms at illness onset are core predictors of functional and clinical outcomes in EOP and would further support the neurodevelopmental nature of psychotic disorders,38 with early-onset forms at one extreme of the continuum of disease severity and genetic liability.39 Indeed, both negative symptoms and premorbid adjustment have also been found to be good predictors of outcome in adult-onset psychosis,40–42 which would support the continuity between EOP and adult-onset psychosis.39 However, as children and adolescents seem to present more frequently with poor premorbid adjustment and greater initial negative symptom severity than adults,43–45 patients with EOP would be at increased risk of poor outcome and should be subject to close monitoring and to early and intensive interventions when required.
The fact that patients with early-onset schizophrenia spectrum disorders usually present with more severe premorbid impairments and initial negative symptoms than other types of EOP8,11–13 could underlie our finding that a diagnosis of schizophrenia predicts greater disability, worse global functioning, and poorer quality of life at follow-up. That being said, it should also be considered that numerous studies have failed to find a significant association between psychosis diagnostic subgroup and functional20,33, 47, 48 or cognitive49–51 outcomes. In addition to potential methodological issues that could underlie these inconsistent findings, it has been proposed that presenting with psychotic symptoms at a young age may be a common phenotypic manifestation of similar deviant neurodevelopmental trajectories in early-onset schizophrenia spectrum disorders and early-onset psychotic bipolar disorder and that differences between the two disorders may be quantitative rather than qualitative in nature.52,53 On the basis of shared genetic vulnerability, having additional neurodevelopmental impairments would shift the phenotypic expression toward more severe presentations that would be associated with worse outcome.54 In keeping with this, poorer outcome would more likely be associated with presence of premorbid impairments or negative symptoms transdiagnostically rather than with a categorical diagnosis of early-onset psychotic bipolar disorder or early-onset schizophrenia spectrum disorders. In fact, when diagnosis, premorbid adjustment and negative symptoms are introduced as independent variables in regression models, premorbid adjustment and baseline negative symptoms are the strongest predictors of functional outcome, accounting together for 55% of the explained variance at 1-year follow-up and for 44% at 2-year follow-up.55 Along those lines, negative symptoms were found to be stronger predictors of functional outcome and of improvement in executive functioning than diagnosis in a prospective cohort of first-episode EOP,29,33 whereas premorbid adjustment was found to be a stronger predictor of functional outcome than diagnosis in a retrospective cohort of EOP.56 These data would further support the relevance of poorer premorbid adjustment and more prominent negative symptoms as markers of more severe outcome in EOP.
Moreover, the association of a diagnosis of schizophrenia with worse outcome should also be appraised in light of the fact that most EOP studies use a follow-up diagnosis to categorize patients into diagnostic subgroups. This strategy can help more accurately define patient diagnosis as it minimizes the impact of diagnostic instability inherent in first episodes of EOP.57 However, if a follow-up diagnosis of schizophrenia is used as a predictor of outcome, there is a risk that those patients showing poorer outcome are also those more likely to receive this diagnosis during follow-up.
Insidious onset and longer DUP are well-replicated predictive factors of worse outcome in EOP in keeping with what has been found in adult-onset psychosis samples.58–61 Indeed, insidious onset is a good predictor of greater illness severity62 and poorer global functioning62–64 at follow-up, whereas longer DUP predicts worse clinical, functional, and cognitive outcomes.29,50 The association between insidious onset and worse outcome may be confounded by the fact that this presentation is also more common in more developmentally impaired patients65 who present poorer outcomes as mentioned above. This may also be the case for DUP, as longer DUP has also been associated with poorer premorbid adjustment.66,67 However, premorbid adjustment and DUP have both been found to be independent predictors of 2-year improvement in functioning in patients with a DUP shorter than 6 months.50 Given that DUP is reported to be longer in EOP than in adult-onset psychosis cases43,44,68 and that it is a potentially modifiable factor, worldwide mental health policies should give priority to early intervention services for children and adolescents, which have proven to be cost effective in this population.69 Such interventions should be considered for numerous psychiatric disorders starting in childhood and adolescence, since reducing the duration of episodes at these developmental stages can positively impact mental health in adulthood.4
Sex and age at onset have yielded inconsistent associations with outcome in EOP, which contrasts with the classical assumption, based on adult-onset studies, that male sex and earlier age at onset are associated with poorer outcomes.70,71 The finding of a worse outcome in adult male patients is frequently contaminated by the fact that males usually have an earlier age at onset and insidious onset.71 In this review, being female was found to be a good predictor of better insight at follow-up and a higher number of readmissions, as well as a significant correlate (by bivariate analyses) of less regional GM loss through follow-up. The lack of a consistent association between sex and outcome in EOP could be due to the fact that females who develop a psychotic disorder during childhood or adolescence probably have a higher load of genetic, neurodevelopmental, or environmental factors leading to significantly earlier onset of the disease in spite of potential protective factors (for example, estrogens). In these individuals, outcome may already be impoverished by the presence of a more severe form of the disorder from the outset. Furthermore, it has also been proposed that prepubertal onset may preclude the protective effect of estrogens on development of the disorder, leading to a more severe course.71 In this review, lower age at onset was found to predict worse quality of psychiatric care and poorer social, educational, and occupational functioning in some multivariate models. However, it was not consistently reported as a significant predictor of functional and other outcomes in other studies using regression models, nor was it a good correlate in studies using bivariate approaches. A narrow age range in studies exclusively including adolescent-onset cases decreases the capability of detecting a significant effect of age at onset. The effect of age at onset (at least in studies using bivariate comparison) seems to be more marked in schizophrenia samples.63,64,72 This may be due to the fact that these are more homogeneous samples in which the contribution of age at onset would be more easily detected than in mixed samples with stronger differences in other relevant predictors (negative symptoms, premorbid functioning), which may obscure the predictive value of age at onset.
Among cognitive predictors of clinical outcomes, lower IQ at baseline was found to predict worse functional outcomes, a diagnostic outcome of schizophrenia, and poorer insight at follow-up in multivariate models, whereas its association with other outcomes such as disability was more inconsistent. Interestingly, higher baseline IQ was found to be a good predictor of functional outcome only for early-onset psychotic bipolar disorder patients in one cohort.56,73 This could be due to a specific effect of IQ in this diagnostic subgroup or to the fact that a higher developmental load in early-onset schizophrenia spectrum disorders may obscure the predictive value of this variable. Other cognitive variables (for example, baseline speed of processing) have been described as good predictors of functional outcomes, but more inconsistently, which highlights the complexity of the interaction between global cognition measures and outcome in EOP and the need to specifically assess the relationship between specific neurocognitive domains and specific dimensions of outcome17,74 or to develop complex predictive models by combining multiple clinical and neuropsychological variables.35 Furthermore, the finding of a strong association between cognition and functional outcome in this review is consistent with results in first episodes of adult-onset schizophrenia, in which cognitive variables and negative symptoms have been found to be the main predictors of long-term functional outcome,74 and points to the potential usefulness of cognitive remediation strategies for improving functional outcome in EOP.75
Although biomarker discovery efforts in psychiatry have gained priority in recent years,76 this review found few studies that focused on the predictive value of biological variables for outcomes in EOP. Lower baseline antioxidant status was found to predict greater loss of GM volume and worse cognitive functioning at follow-up in one cohort.77,78 These findings provide some support for the role of oxidative stress in EOP79 warranting further replication. These findings may also point to the potential applicability of antioxidant strategies to the treatment of EOP patients, as suggested by the promising results of a developmental animal model of schizophrenia indicating that the use of N-acetylcysteine can prevent the later expression of schizophrenia-like traits in adulthood.80 Among neuroimaging markers, cortical thickness and GM volume at baseline in different brain regions were reported to significantly predict remission81 and insight82 at follow-up, respectively, in studies using multivariate models. These are also findings with high potential for translational applicability warranting further replication. Even if implementation of biological predictors in psychiatric settings is still a way off, assessment of their predictive value is warranted by complex predictive models in combination with other relevant clinical, functional, and cognitive variables on a subject-by-subject basis using novel multivariate machine-learning methods. This could help design personalized medicine models by stratifying patients according to their risk of poor outcome or treatment response. These models would help determine whether more intensive interventions (for example, earlier initiation of clozapine treatment or more intensive psychosocial support) would be justified for a defined subset of EOP patients, an issue of great clinical and economic importance as this could improve quality of life in patients with EOP and reduce the burden of disease and cost to national health systems.
This work is subject to several caveats. First, differing outcome measures, length of follow-up, outcome measures, and designs make it difficult to compare studies. Many studies used a retrospective design, with retrospective identification of cases and use of clinical records for assessment of baseline variables. The lack of standardized data-recording methods may have led to inaccuracy or inconsistent reporting of different predictors. Furthermore, attrition rates were high in most of the studies, which may have affected the results to some extent, since it is usually difficult to establish whether discontinuation is due to factors such as lack of compliance or more severe course. Although many studies used appropriate statistical methods to identify predictors, most of the older studies provided only descriptive data and bivariate comparisons between potentially relevant variables, which precluded assessing the impact of potential covariates in the results. This is illustrated by studies finding significant results in bivariate comparisons that do not survive regression analyses.26 That being said, given the scarcity of studies on EOP and relevant outcomes, studies using traditional bivariate comparisons were ultimately included in this review so as to acquire a broader view of the issue. It should also be considered that our findings from multivariate models may have been influenced by the covariates introduced into the models, which differed among studies and were rarely selected systematically. Furthermore, the inclusion of studies using different diagnostic criteria (see Methods) may have also affected our findings to some extent. However, all patients included in this review were diagnosed or re-diagnosed with at least the DSM-III-R, whose diagnostic criteria for psychotic disorders are similar to those of current classification systems. Second, since findings on neurobiological predictors are mostly based on single studies, further replication would be needed to support their predictive value. Third, the exclusion of results based on clinical trials from this review may have prevented us from detecting some significant predictors of treatment response or short-term adherence. For example, data from a 6-month clinical trial found that a better attitude toward antipsychotic medication at a first lifetime psychiatric admission for a first early-onset psychotic episode was significantly related to lower all-cause antipsychotic treatment discontinuation.46 However, we decided not to include results from clinical trials to ascertain predictors of outcome over the course of EOP not related to specific therapeutic interventions.
These limitations notwithstanding, this is to the best of our knowledge the first systematic review to provide a comprehensive overview of recent studies on predictors of clinical, functional, cognitive, and neurobiological outcomes in EOP. Accurate research with potential for replication based on long-term longitudinal studies targeting the search for such predictors is needed.83 This could help identify subjects with EOP at higher risk of poor outcome in whom more intensive and earlier interventions would be warranted. Early intervention services in EOP should aim at shortening DUP and at carefully monitoring patients with poorer adjustment and more severe negative symptoms at first presentation. Novel therapeutic approaches targeting negative and cognitive symptoms are needed to improve the outcome of EOP.
References
Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C et al. Global burden of disease in young people aged 10-24 years: a systematic analysis. Lancet 2011; 377: 2093–2102.
Madhusoodanan S . Preventive psychiatry: we are getting closer to fulfilling the promise of reducing mental illness. Ann Clin Psychiatry 2010; 22: 217–218.
McGorry PD . Risk syndromes, clinical staging and DSM V: new diagnostic infrastructure for early intervention in psychiatry. Schizophr Res 2010; 120: 49–53.
Patton GC, Coffey C, Romaniuk H, Mackinnon A, Carlin JB, Degenhardt L et al. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet 2014; 383: 1404–1411.
Hazell P . Does the treatment of mental disorders in childhood lead to a healthier adulthood? Curr Opin Psychiatry 2007; 20: 315–318.
McFarlane WR, Levin B, Travis L, Lucas FL, Lynch S, Verdi M et al. Clinical and functional outcomes after 2 years in the early detection and intervention for the prevention of psychosis multisite effectiveness trial. Schizophr Bull 2015; 41: 30–43.
Francey SM, Nelson B, Thompson A, Parker AG, Kerr M, Macneil C et al. Who needs antipsychotic medication in the earliest stages of psychosis? A reconsideration of benefits, risks, neurobiology and ethics in the era of early intervention. Schizophr Res 2010; 119: 1–10.
de Girolamo G, Dagani J, Purcell R, Cocchi A, McGorry PD . Age of onset of mental disorders and use of mental health services: needs, opportunities and obstacles. Epidemiol Psychiatr Sci 2012; 21: 47–57.
Beardslee WR, Brent DA, Weersing VR, Clarke GN, Porta G, Hollon SD et al. Prevention of depression in at-risk adolescents: longer-term effects. JAMA Psychiatry 2013; 70: 1161–1170.
Schimmelmann BG, Conus P, Cotton S, McGorry PD, Lambert M . Pre-treatment, baseline, and outcome differences between early-onset and adult-onset psychosis in an epidemiological cohort of 636 first-episode patients. Schizophr Res 2007; 95: 1–8.
Amminger GP, Henry LP, Harrigan SM, Harris MG, Alvarez-Jimenez M, Herrman H et al. Outcome in early-onset schizophrenia revisited: findings from the Early Psychosis Prevention and Intervention Centre long-term follow-up study. Schizophr Res 2011; 131: 112–119.
Hafner H, Nowotny B . Epidemiology of early-onset schizophrenia. Eur Arch Psychiatry Clin Neurosci 1995; 245: 80–92.
Clemmensen L, Vernal DL, Steinhausen HC . A systematic review of the long-term outcome of early onset schizophrenia. BMC Psychiatry 2012; 12: 150.
Zipursky RB, Reilly TJ, Murray RM . The myth of schizophrenia as a progressive brain disease. Schizophr Bull 2013; 39: 1363–1372.
Wunderink L, Nieboer RM, Wiersma D, Sytema S, Nienhuis FJ . Recovery in remitted first-episode psychosis at 7 years of follow-up of an early dose reduction/discontinuation or maintenance treatment strategy: long-term follow-up of a 2-year randomized clinical trial. JAMA Psychiatry 2013; 70: 913–920.
Menezes NM, Milovan E . First-episode psychosis: a comparative review of diagnostic evolution and predictive variables in adolescents versus adults. Can J Psychiatry 2000; 45: 710–716.
Remschmidt H, Theisen F . Early-onset schizophrenia. Neuropsychobiology 2012; 66: 63–69.
Moher D, Liberati A, Tetzlaff J, Altman DG . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009; 339: b2535.
Rutter M . Childhood schizophrenia reconsidered. J Autism Child Schizophr 1972; 2: 315–337.
Gillberg IC, Hellgren L, Gillberg C . Psychotic disorders diagnosed in adolescence. Outcome at age 30 years. J Child Psychol Psychiatry 1993; 34: 1173–1185.
Remberk B, Bazynska AK, Krempa-Kowalewska A, Rybakowski F . Adolescent insanity revisited: course and outcome in early-onset schizophrenia spectrum psychoses in an 8-year follow-up study. Compr Psychiatry 2014; 55: 1174–1181.
Paillere-Martinot ML, Aubin F, Martinot JL, Colin B . A prognostic study of clinical dimensions in adolescent-onset psychoses. Schizophr Bull 2000; 26: 789–799.
Bachman P, Niendam TA, Jalbrzikowski M, Park CY, Daley M, Cannon TD et al. Processing speed and neurodevelopment in adolescent-onset psychosis: cognitive slowing predicts social function. J Abnorm Child Psychol 2012; 40: 645–654.
Valevski A, Ratzoni G, Sever J, Apter A, Zalsman G, Shiloh R et al. Stability of diagnosis: a 20-year retrospective cohort study of Israeli psychiatric adolescent inpatients. J Adolesc 2001; 24: 625–633.
Pencer A, Addington J, Addington D . Outcome of a first episode of psychosis in adolescence: a 2-year follow-up. Psychiatry Res 2005; 133: 35–43.
Hassan GA, Taha GR . Long term functioning in early onset psychosis: two years prospective follow-up study. Behav Brain Funct 2011; 7: 28.
Maziade M, Gingras N, Rodrigue C, Bouchard S, Cardinal A, Gauthier B et al. Long-term stability of diagnosis and symptom dimensions in a systematic sample of patients with onset of schizophrenia in childhood and early adolescence. I: nosology, sex and age of onset. Br J Psychiatry 1996; 169: 361–370.
Meng H, Schimmelmann BG, Mohler B, Lambert M, Branik E, Koch E et al. Pretreatment social functioning predicts 1-year outcome in early onset psychosis. Acta Psychiatr Scand 2006; 114: 249–256.
Fraguas D, Merchan-Naranjo J, Del Rey-Mejias A, Castro-Fornieles J, Gonzalez-Pinto A, Rapado-Castro M et al. A longitudinal study on the relationship between duration of untreated psychosis and executive function in early-onset first-episode psychosis. Schizophr Res 2014; 158: 126–133.
Lay B, Blanz B, Hartmann M, Schmidt MH . The psychosocial outcome of adolescent-onset schizophrenia: a 12-year followup. Schizophr Bull 2000; 26: 801–816.
Krausz M, Muller-Thomsen T . Schizophrenia with onset in adolescence: an 11-year followup. Schizophr Bull 1993; 19: 831–841.
Reichert A, Kreiker S, Mehler-Wex C, Warnke A . The psychopathological and psychosocial outcome of early-onset schizophrenia: preliminary data of a 13-year follow-up. Child Adolesc Psychiatry Ment Health 2008; 2: 6.
Fraguas D, de Castro MJ, Medina O, Parellada M, Moreno D, Graell M et al. Does diagnostic classification of early-onset psychosis change over follow-up? Child Psychiatry Hum Dev 2008; 39: 137–145.
Aarkrog T . Psychotic adolescents 20–25 years later. Nord J Psychiatry 1999; 53 (Suppl 42(i-viii)): 1–38.
Pina-Camacho L, Garcia-Prieto J, Parellada M, Castro-Fornieles J, Gonzalez-Pinto AM, Bombin I et al. Predictors of schizophrenia spectrum disorders in early-onset first episodes of psychosis: a support vector machine model. Eur Child Adolesc Psychiatry 2014 Aug 11. [Epub ahead of print]. 10.1007/s00787-014-0593-0.
Hollis C . Developmental precursors of child- and adolescent-onset schizophrenia and affective psychoses: diagnostic specificity and continuity with symptom dimensions. Br J Psychiatry 2003; 182: 37–44.
Strauss GP, Allen DN, Miski P, Buchanan RW, Kirkpatrick B, Carpenter WT Jr . Differential patterns of premorbid social and academic deterioration in deficit and nondeficit schizophrenia. Schizophr Res 2012; 135: 134–138.
Owen MJ, O'Donovan MC, Thapar A, Craddock N . Neurodevelopmental hypothesis of schizophrenia. Br J Psychiatry 2011; 198: 173–175.
Hollis C . Adult outcomes of child- and adolescent-onset schizophrenia: diagnostic stability and predictive validity. Am J Psychiatry 2000; 157: 1652–1659.
Lang FU, Kosters M, Lang S, Becker T, Jager M . Psychopathological long-term outcome of schizophrenia -- a review. Acta Psychiatr Scand 2013; 127: 173–182.
Chang WC, Tang JY, Hui CL, Wong GH, Chan SK, Lee EH et al. The relationship of early premorbid adjustment with negative symptoms and cognitive functions in first-episode schizophrenia: a prospective three-year follow-up study. Psychiatry Res 2013; 209: 353–360.
McGlashan TH . The prediction of outcome in chronic schizophrenia. IV. The Chestnut Lodge follow-up study. Arch Gen Psychiatry 1986; 43: 167–176.
Ballageer T, Malla A, Manchanda R, Takhar J, Haricharan R . Is adolescent-onset first-episode psychosis different from adult onset? J Am Acad Child Adolesc Psychiatry 2005; 44: 782–789.
Joa I, Johannessen JO, Langeveld J, Friis S, Melle I, Opjordsmoen S et al. Baseline profiles of adolescent vs. adult-onset first-episode psychosis in an early detection program. Acta Psychiatr Scand 2009; 119: 494–500.
Vourdas A, Pipe R, Corrigall R, Frangou S . Increased developmental deviance and premorbid dysfunction in early onset schizophrenia. Schizophr Res 2003; 62: 13–22.
Fraguas D, Llorente C, Rapado-Castro M, Parellada M, Moreno D, Ruiz-Sancho A et al. Attitude toward antipsychotic medication as a predictor of antipsychotic treatment discontinuation in first-episode early-onset psychosis. Rev Psiquiatr Salud Ment 2008; 1: 10–17.
McClellan JM, Werry JS, Ham M . A follow-up study of early onset psychosis: comparison between outcome diagnoses of schizophrenia, mood disorders, and personality disorders. J Autism Dev Disord 1993; 23: 243–262.
Lay B, Schmidt MH, Blanz B . Course of adolescent psychotic disorder with schizoaffective episodes. Eur Child Adolesc Psychiatry 1997; 6: 32–41.
Bombin I, Mayoral M, Castro-Fornieles J, Gonzalez-Pinto A, de la Serna E, Rapado-Castro M et al. Neuropsychological evidence for abnormal neurodevelopment associated with early-onset psychoses. Psychol Med 2013; 43: 757–768.
Fraguas D, Del Rey-Mejias A, Moreno C, Castro-Fornieles J, Graell M, Otero S et al. Duration of untreated psychosis predicts functional and clinical outcome in children and adolescents with first-episode psychosis: a 2-year longitudinal study. Schizophr Res 2014; 152: 130–138.
Jepsen JR, Fagerlund B, Pagsberg AK, Christensen AM, Hilker RW, Nordentoft M et al. Course of intelligence deficits in early onset, first episode schizophrenia: a controlled, 5-year longitudinal study. Eur Child Adolesc Psychiatry 2010; 19: 341–351.
Arango C, Fraguas D, Parellada M . Differential neurodevelopmental trajectories in patients with early-onset bipolar and schizophrenia disorders. Schizophr Bull 2014; 40 (Suppl 2): S138–S146.
Janssen J, Aleman-Gomez Y, Schnack H, Balaban E, Pina-Camacho L, Alfaro-Almagro F et al. Cortical morphology of adolescents with bipolar disorder and with schizophrenia. Schizophr Res 2014; 158: 91–99.
Demjaha A, MacCabe JH, Murray RM . How genes and environmental factors determine the different neurodevelopmental trajectories of schizophrenia and bipolar disorder. Schizophr Bull 2012; 38: 209–214.
McClellan J, McCurry C, Snell J, DuBose A . Early-onset psychotic disorders: course and outcome over a 2-year period. J Am Acad Child Adolesc Psychiatry 1999; 38: 1380–1388.
Werry JS, McClellan JM . Predicting outcome in child and adolescent (early onset) schizophrenia and bipolar disorder. J Am Acad Child Adolesc Psychiatry 1992; 31: 147–150.
Castro-Fornieles J, Baeza I, de la Serna E, Gonzalez-Pinto A, Parellada M, Graell M et al. Two-year diagnostic stability in early-onset first-episode psychosis. J Child Psychol Psychiatry 2011; 52: 1089–1098.
Juola P, Miettunen J, Veijola J, Isohanni M, Jaaskelainen E . Predictors of short- and long-term clinical outcome in schizophrenic psychosis--the Northern Finland 1966 Birth Cohort study. Eur Psychiatry 2013; 28: 263–268.
Marshall M, Lewis S, Lockwood A, Drake R, Jones P, Croudace T . Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychiatry 2005; 62: 975–983.
Perkins DO, Gu H, Boteva K, Lieberman JA . Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: a critical review and meta-analysis. Am J Psychiatry 2005; 162: 1785–1804.
Penttila M, Jaaskelainen E, Hirvonen N, Isohanni M, Miettunen J . Duration of untreated psychosis as predictor of long-term outcome in schizophrenia: systematic review and meta-analysis. Br J Psychiatry 2014; 205: 88–94.
Ropcke B, Eggers C . Early-onset schizophrenia: a 15-year follow-up. Eur Child Adolesc Psychiatry 2005; 14: 341–350.
Kydd RR, Werry JS . Schizophrenia in children under 16 years. J Autism Dev Disord 1982; 12: 343–357.
Fleischhaker C, Schulz E, Tepper K, Martin M, Hennighausen K, Remschmidt H . Long-term course of adolescent schizophrenia. Schizophr Bull 2005; 31: 769–780.
Strous RD, Alvir JM, Robinson D, Gal G, Sheitman B, Chakos M et al. Premorbid functioning in schizophrenia: relation to baseline symptoms, treatment response, and medication side effects. Schizophr Bull 2004; 30: 265–278.
Jeppesen P, Petersen L, Thorup A, Abel MB, Ohlenschlaeger J, Christensen TO et al. The association between pre-morbid adjustment, duration of untreated psychosis and outcome in first-episode psychosis. Psychol Med 2008; 38: 1157–1166.
Verdoux H, Liraud F, Bergey C, Assens F, Abalan F, van Os J . Is the association between duration of untreated psychosis and outcome confounded? A two year follow-up study of first-admitted patients. Schizophr Res 2001; 49: 231–241.
Dominguez MD, Fisher HL, Major B, Chisholm B, Rahaman N, Joyce J et al. Duration of untreated psychosis in adolescents: ethnic differences and clinical profiles. Schizophr Res 2013; 150: 526–532.
McCrone P, Singh SP, Knapp M, Smith J, Clark M, Shiers D et al. The economic impact of early intervention in psychosis services for children and adolescents. Early Interv Psychiatry 2013; 7: 368–373.
Hafner H . Gender differences in schizophrenia. Psychoneuroendocrinology 2003; 28 (Suppl 2): 17–54.
Hafner H, Maurer K, Loffler W, Riecher-Rossler A . The influence of age and sex on the onset and early course of schizophrenia. Br J Psychiatry 1993; 162: 80–86.
Eggers C, Bunk D . The long-term course of childhood-onset schizophrenia: a 42-year followup. Schizophr Bull 1997; 23: 105–117.
Werry JS, McClellan JM, Chard L . Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: a clinical and outcome study. J Am Acad Child Adolesc Psychiatry 1991; 30: 457–465.
Milev P, Ho BC, Arndt S, Andreasen NC . Predictive values of neurocognition and negative symptoms on functional outcome in schizophrenia: a longitudinal first-episode study with 7-year follow-up. Am J Psychiatry 2005; 162: 495–506.
Puig O, Penades R, Baeza I, De la Serna E, Sanchez-Gistau V, Bernardo M et al. Cognitive remediation therapy in adolescents with early-onset schizophrenia: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry 2014; 53: 859–868.
Singh I, Rose N . Biomarkers in psychiatry. Nature 2009; 460: 202–207.
Fraguas D, Gonzalez-Pinto A, Mico JA, Reig S, Parellada M, Martinez-Cengotitabengoa M et al. Decreased glutathione levels predict loss of brain volume in children and adolescents with first-episode psychosis in a two-year longitudinal study. Schizophr Res 2012; 137: 58–65.
Martinez-Cengotitabengoa M, Mico JA, Arango C, Castro-Fornieles J, Graell M, Paya B et al. Basal low antioxidant capacity correlates with cognitive deficits in early onset psychosis. A 2-year follow-up study. Schizophr Res 2014; 156: 23–29.
Mico JA, Rojas-Corrales MO, Gibert-Rahola J, Parellada M, Moreno D, Fraguas D et al. Reduced antioxidant defense in early onset first-episode psychosis: a case-control study. BMC Psychiatry 2011; 11: 26.
Cabungcal JH, Counotte DS, Lewis EM, Tejeda HA, Piantadosi P, Pollock C et al. Juvenile antioxidant treatment prevents adult deficits in a developmental model of schizophrenia. Neuron 2014; 83: 1073–1084.
Greenstein DK, Wolfe S, Gochman P, Rapoport JL, Gogtay N . Remission status and cortical thickness in childhood-onset schizophrenia. J Am Acad Child Adolesc Psychiatry 2008; 47: 1133–1140.
Parellada M, Boada L, Fraguas D, Reig S, Castro-Fornieles J, Moreno D et al. Trait and state attributes of insight in first episodes of early-onset schizophrenia and other psychoses: a 2-year longitudinal study. Schizophr Bull 2011; 37: 38–51.
Castro-Fornieles J . Child and adolescent psychiatry: the need for training and development. Rev Psiquiatr Salud Ment 2013; 6: 57–59.
Ledda MG, Fratta AL, Pintor M, Zuddas A, Cianchetti C . Early-onset psychoses: comparison of clinical features and adult outcome in 3 diagnostic groups. Child Psychiatry Hum Dev 2009; 40: 421–437.
Janssen J, Reig S, Parellada M, Moreno D, Graell M, Fraguas D et al. Regional gray matter volume deficits in adolescents with first-episode psychosis. J Am Acad Child Adolesc Psychiatry 2008; 47: 1311–1320.
Maziade M, Bouchard S, Gingras N, Charron L, Cardinal A, Roy MA et al. Long-term stability of diagnosis and symptom dimensions in a systematic sample of patients with onset of schizophrenia in childhood and early adolescence. II: Postnegative distinction and childhood predictors of adult outcome. Br J Psychiatry 1996; 169: 371–378.
Jarbin H, Hansson L . Adult quality of life and associated factors in adolescent onset schizophrenia and affective psychotic disorders. Soc Psychiatry Psychiatr Epidemiol 2004; 39: 725–729.
Bunk D, Eggers C, Volberg G, Schebaum-Stein T . Dimensions of premorbid disorders in childhood-onset schizophrenia (COS). Neurol Psychiatry Brain Res 2003; 10: 183–192.
Baeza I, Graell M, Moreno D, Castro-Fornieles J, Parellada M, Gonzalez-Pinto A et al. Cannabis use in children and adolescents with first episode psychosis: influence on psychopathology and short-term outcome (CAFEPS study). Schizophr Res 2009; 113: 129–137.
Wozniak JR, Block EE, White T, Jensen JB, Schulz SC . Clinical and neurocognitive course in early-onset psychosis: a longitudinal study of adolescents with schizophrenia-spectrum disorders. Early Interv Psychiatry 2008; 2: 169–177.
Mayoral M, Zabala A, Robles O, Bombin I, Andres P, Parellada M et al. Neuropsychological functioning in adolescents with first episode psychosis: a two-year follow-up study. Eur Psychiatry 2008; 23: 375–383.
Cawthron P, James A, Dell J, Seagroatt V . Adolescent onset psychosis. A clinical and outcome study. J Child Psychol Psychiatry 1994; 35: 1321–1332.
Eggers C, Bunk D, Volberg G, Ropcke B . The ESSEN study of childhood-onset schizophrenia: selected results. Eur Child Adolesc Psychiatry 1999; 8 (Suppl 1): I21–I28.
Schimmelmann BG, Conus P, Cotton S, Kupferschmid S, McGorry PD, Lambert M . Prevalence and impact of cannabis use disorders in adolescents with early onset first episode psychosis. Eur Psychiatry 2012; 27: 463–469.
Amminger GP, Resch F, Mutschlechner R, Friedrich MH, Ernst E . Premorbid adjustment and remission of positive symptoms in first-episode psychosis. Eur Child Adolesc Psychiatry 1997; 6: 212–218.
Gearing RE, Mian I, Sholonsky A, Barber J, Nicholas D, Lewis R et al. Developing a risk-model of time to first-relapse for children and adolescents with a psychotic disorder. J Nerv Ment Dis 2009; 197: 6–14.
Jarbin H, Grawe RW, Hansson K . Expressed emotion and prediction of relapse in adolescents with psychotic disorders. Nord J Psychiatry 2000; 54: 201–205.
Gearing RE, Charach A . Medication adherence for children and adolescents with first-episode psychosis following hospitalization. Eur Child Adolesc Psychiatry 2009; 18: 587–595.
Noguera A, Ballesta P, Baeza I, Arango C, de la Serna E, Gonzalez-Pinto A et al. Twenty-four months of antipsychotic treatment in children and adolescents with first psychotic episode: discontinuation and tolerability. J Clin Psychopharmacol 2013; 33: 463–471.
Parellada M, Fraguas D, Bombin I, Otero S, Castro-Fornieles J, Baeza I et al. Insight correlates in child- and adolescent-onset first episodes of psychosis: results from the CAFEPS study. Psychol Med 2009; 39: 1433–1445.
Sanchez-Gistau V, Baeza I, Arango C, Gonzalez-Pinto A, de la Serna E, Parellada M et al. Predictors of suicide attempt in early-onset, first-episode psychoses: a longitudinal 24-month follow-up study. J Clin Psychiatry 2013; 74: 59–66.
Jarbin H, Von Knorring AL . Suicide and suicide attempts in adolescent-onset psychotic disorders. Nord J Psychiatry 2004; 58: 115–123.
Jarbin H, Ott Y, Von Knorring AL . Adult outcome of social function in adolescent-onset schizophrenia and affective psychosis. J Am Acad Child Adolesc Psychiatry 2003; 42: 176–183.
Werry JS, McClellan JM, Andrews LK, Ham M . Clinical features and outcome of child and adolescent schizophrenia. Schizophr Bull 1994; 20: 619–630.
Sporn AL, Vermani A, Greenstein DK, Bobb AJ, Spencer EP, Clasen LS et al. Clozapine treatment of childhood-onset schizophrenia: evaluation of effectiveness, adverse effects, and long-term outcome. J Am Acad Child Adolesc Psychiatry 2007; 46: 1349–1356.
McClellan J, McCurry C, Speltz ML, Jones K . Symptom factors in early-onset psychotic disorders. J Am Acad Child Adolesc Psychiatry 2002; 41: 791–798.
Remschmidt H, Martin M, Fleischhaker C, Theisen FM, Hennighausen K, Gutenbrunner C et al. Forty-two-years later: the outcome of childhood-onset schizophrenia. J Neural Transm 2007; 114: 505–512.
Vyas NS, Hadjulis M, Vourdas A, Byrne P, Frangou S . The Maudsley early onset schizophrenia study. Predictors of psychosocial outcome at 4-year follow-up. Eur Child Adolesc Psychiatry 2007; 16: 465–470.
Oie M, Sundet K, Ueland T . Neurocognition and functional outcome in early-onset schizophrenia and attention-deficit/hyperactivity disorder: a 13-year follow-up. Neuropsychology 2011; 25: 25–35.
Cervellione KL, Burdick KE, Cottone JG, Rhinewine JP, Kumra S . Neurocognitive deficits in adolescents with schizophrenia: longitudinal stability and predictive utility for short-term functional outcome. J Am Acad Child Adolesc Psychiatry 2007; 46: 867–878.
Schmidt M, Blanz B, Dippe A, Koppe T, Lay B . Course of patients diagnosed as having schizophrenia during first episode occurring under age 18 years. Eur Arch Psychiatry Clin Neurosci 1995; 245: 93–100.
de la Serna E, Andres-Perpina S, Puig O, Baeza I, Bombin I, Bartres-Faz D et al. Cognitive reserve as a predictor of two year neuropsychological performance in early onset first-episode schizophrenia. Schizophr Res 2013; 143: 125–131.
Thompson PM, Vidal C, Giedd JN, Gochman P, Blumenthal J, Nicolson R et al. Mapping adolescent brain change reveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia. Proc Natl Acad Sci USA 2001; 98: 11650–11655.
Arango C, Rapado-Castro M, Reig S, Castro-Fornieles J, Gonzalez-Pinto A, Otero S et al. Progressive brain changes in children and adolescents with first-episode psychosis. Arch Gen Psychiatry 2012; 69: 16–26.
Sporn AL, Greenstein DK, Gogtay N, Jeffries NO, Lenane M, Gochman P et al. Progressive brain volume loss during adolescence in childhood-onset schizophrenia. Am J Psychiatry 2003; 160: 2181–2189.
Rapoport JL, Giedd JN, Blumenthal J, Hamburger S, Jeffries N, Fernandez T et al. Progressive cortical change during adolescence in childhood-onset schizophrenia. A longitudinal magnetic resonance imaging study. Arch Gen Psychiatry 1999; 56: 649–654.
Gogtay N, Sporn A, Clasen LS, Nugent TF 3rd, Greenstein D, Nicolson R et al. Comparison of progressive cortical gray matter loss in childhood-onset schizophrenia with that in childhood-onset atypical psychoses. Arch Gen Psychiatry 2004; 61: 17–22.
Jacobsen LK, Giedd JN, Castellanos FX, Vaituzis AC, Hamburger SD, Kumra S et al. Progressive reduction of temporal lobe structures in childhood-onset schizophrenia. Am J Psychiatry 1998; 155: 678–685.
Acknowledgements
Funding
This study was supported by the Spanish Ministry of Economy and Competitiveness, Instituto de Salud Carlos III (FIS PS09/01442 and PI12/1303), CIBERSAM, Madrid Regional Government (S2010/BMD-2422 AGES), European Union Structural Funds and European Union Seventh Framework Programme under grant agreements FP7-HEALTH-2009-2.2.1-2-241909 (Project EU-GEI), FP7-HEALTH-2009-2.2.1-3-242114 (Project OPTiMISE), FP7-HEALTH-2013-2.2.1-2-603196 (Project PSYSCAN), and FP7-HEALTH-2013-2.2.1-2-602478 (Project METSY); Fundación Alicia Koplowitz (FAK2012, FAK2013), Fundación Mutua Madrileña (FMM2009), and ERA-NET NEURON (Network of European Funding for Neuroscience Research) (PIM2010ERN-00642). CMD-C has previously held a Río Hortega grant, Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness, and a grant from Fundación Alicia Koplowitz. LP-C holds a grant from Fundación Alicia Koplowitz and has previously held a Río Hortega grant, Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness. AR-Q holds a Río Hortega grant, Instituto de Salud Carlos III, Spanish Ministry of Economy and Competitiveness.
Author information
Authors and Affiliations
Contributions
All authors contributed to the protocol for this work. CMD-C, LP-C, and AR-Q performed the literature review and the selection of references. CMD-C and AR-Q extracted the data. CMD-C and LP-C wrote the first draft of the manuscript, which was subsequently edited by all authors, who contributed to the interpretation of the findings and approved the final version. All authors had full access to the data and take responsibility for their integrity and accuracy.
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Díaz-Caneja, C., Pina-Camacho, L., Rodríguez-Quiroga, A. et al. Predictors of outcome in early-onset psychosis: a systematic review. npj Schizophr 1, 14005 (2015). https://doi.org/10.1038/npjschz.2014.5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/npjschz.2014.5
This article is cited by
-
Relationship between social cognition and premorbid adjustment in psychosis: a systematic review
Schizophrenia (2024)
-
Challenges and opportunities in the diagnosis and treatment of early-onset psychosis: a case series from the youth affective disorders clinic in Stockholm, Sweden
Schizophrenia (2024)
-
Neurocognition and functioning in adolescents at clinical high risk for psychosis
Child and Adolescent Psychiatry and Mental Health (2023)
-
Could psychedelic drugs have a role in the treatment of schizophrenia? Rationale and strategy for safe implementation
Molecular Psychiatry (2023)
-
Risk and protective factors for recovery at 3-year follow-up after first-episode psychosis onset: a multivariate outcome approach
Social Psychiatry and Psychiatric Epidemiology (2023)
